不想錯過界哥的推送?
↑戳上方藍字「醫學界內分泌頻道」關注我們
並點擊右上角「···」目錄,選擇「設為星標」


分化型甲狀腺癌,從評估到隨訪,4張表、3張圖、6件事,1篇文章徹底說清楚!
作者 | 鯨魚
來源 | 醫學界內分泌頻道
本文提要
風險評估:四張表、五個因素
隨訪計劃:三張圖、三種情況
畫個重點:六件事、一文搞定
甲狀腺癌是最常見的內分泌惡性腫瘤,佔所有癌症發病的3%。96%的甲狀腺癌來自於濾泡細胞,其中99%為分化型甲狀腺癌(differentiated thyroid cancer, DTC),包括乳頭狀癌(papillary thyroid cancer, PTC)、濾泡狀癌(follicular thyroid cancer, FTC)、Hürthle細胞癌(Hürthle cell carcinoma, HCC)和分化較差的甲狀腺癌(poorly differentiated thyroid cancer, PDTC)[1]。

近年來,DTC的發病率不斷上升,過度診斷、輻射暴露、肥胖均有可能與之相關[3,4]。由於患病人數的不斷增加,其治療也越來越受到人們的關注。過去,DTC的治療常常是一刀切,甲狀腺全切、放射性碘殘餘灶清掃、左旋甲狀腺素抑製促甲狀腺素(thyroid stimulating hormone, TSH)[5]——這種按部就班的處理方式還是適用於高危的DTC,但絕大多數DTC的複發風險較低,需要更為個體化的治療。


Fig 0.2 綜述8月1日發表在Nature Reviews Endocrinology[6]
最近,Nature Reviews Endocrinology上的一篇綜述《分化型甲狀腺癌的隨訪:那些該做的和不該做的》就針對這一情況,闡述了DTC的初始治療、監測手段和隨訪策略的優缺點,討論了風險分層評估工具、隨訪檢測的手段和個體化隨訪計劃的制定[6]。
一
風險評估:四張表、五個因素
甲狀腺癌隨訪計劃的製訂需要由甲狀腺癌的分期、複發風險、對治療的反應、組織類型、分子分型等因素共同決定。

對於甲狀腺癌,通常會使用美國癌症聯合委員會和國際抗癌聯盟(American Joint Committee on Cancer and Union Internationale Contre le Cancer, AJCC-UICC)的腫瘤淋巴結轉移分期系統進行分期,該分期系統在2017年更新到了第8版。
Tab. 1 AJCC-TNM 第7/8版本甲狀腺癌分期[7-9]


Tab. 2 ATA 甲狀腺癌複發風險[10-12]


Tab. 3 患者對治療的反應[10,12,14]


Tab. 4 頸部淋巴結惡性可疑的超聲徵象[15-17]



此外,甲狀腺癌的組織學分型和分子分型對於其隨訪計劃的製訂也很有價值[6]。比如,甲狀腺乳頭狀癌及濾泡狀癌通常預後較好,可以選擇較為寬鬆的隨訪計劃,但其中侵襲性更強的亞型以及Hürthle細胞癌和分化較差的甲狀腺癌的預後通常較差,因此需要更嚴密的隨訪。


腫瘤的分子分型也有助於識別需要更頻繁隨訪的高風險亞型,常見的基因變異如BRAFV600E、RAS等對於治療的選擇也有很大意義。
二
隨訪計劃:三張圖、三種情況
在甲狀腺癌的隨訪中,綜述提出了可以使用的5個工具,分別為血清Tg、Tg-Ab水準、頸部超聲及細胞學檢查、全身放射性碘掃描和包括CT、MRI、18F-FDG–PET、18F-FDG–PET–CT在內的多種橫斷面及功能成像[6]。這些手段的不同組合形成了針對不同風險人群的隨訪計劃。

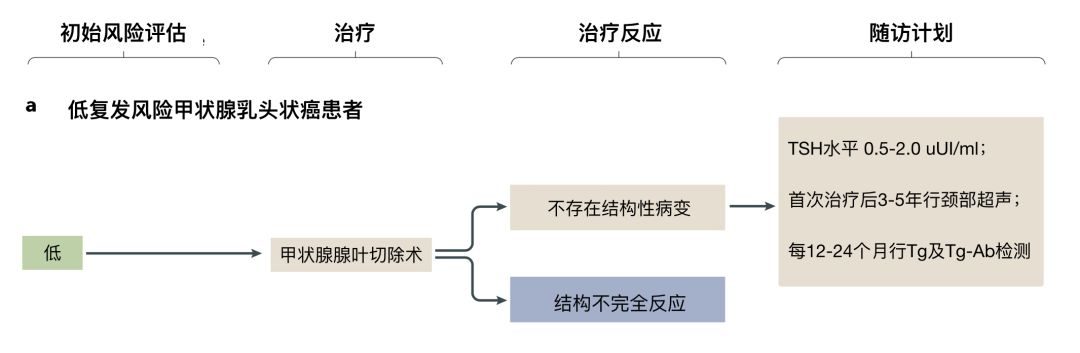
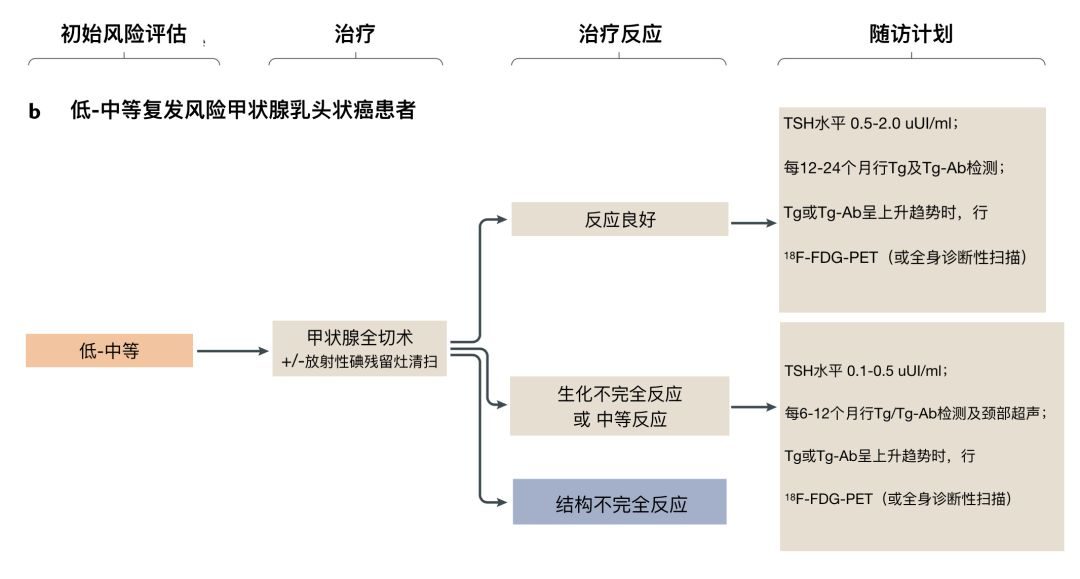



不過,綜述也指出,由於缺乏明確、直接的指導意見,這些隨訪計劃的變化性很大,受到各個地區的條件、臨床醫生和患者偏好的影響[6]。
三
畫個重點:六件事、一文搞定
總的來說,分化型甲狀腺癌患者可以使用多種隨訪工具,但對於大多數患者,也就是那些對治療反應良好並且中低複發風險的患者來說,非常簡單的隨訪計劃就已經足夠。
這一計劃可能包括:持續5年每年測定血清TSH、Tg和Tg-Ab水準,隨後改為每2年一次測定,並且僅對發現這些指標異常的患者行頸部超聲檢查。而有中高風險的患者則應該有選擇地接受更頻繁評估以及超聲之外的二線影像學檢查手段。另外,基於分子分型的數據能更精準地預測腫瘤風險,朝著精準醫學邁出重要一步。


說了這麼多,最後來劃個重點!
-
1. 甲狀腺癌的隨訪計劃要根據其組織學類型、初始治療、初始複發風險和對治療的反應來決定;
-
2. 對初始治療反應良好是指,在檢測不到Tg-Ab、頸部超聲檢查也沒有異常發現的情況下,檢測不到Tg;
-
3. 對治療有反應良好、低或中等複發風險患者,每年隨訪檢測血清TSH、Tg和Tg-Ab;
-
4. 當血清Tg或Tg-Ab水準隨時間呈上升趨勢時,應該根據患者的複發風險和當地資源來考慮進行超聲檢查、橫斷面成像或功能成像;
-
5. 對治療反應不佳的高複發風險患者,應每6~12個月隨訪血清TSH、Tg和Tg-Ab以及頸部超聲;
6. 未治療時,應定期對結構性病變進行隨訪,隨訪頻率和影像學工具的選擇取決於疾病負擔、進展、位置和速度。
—————
Related Articles
[1] 救救甲狀腺!NEJM:甲狀腺微小乳頭狀癌,別上來就是一刀!
[2] 甲亢、甲減,多一「碘」還是少一「碘」?
[3] 偶然發現甲狀腺結節怎麼辦?頂級期刊CA這樣說!
REF:
[1] Fagin JA, Wells SA Jr. (2016). Biologic and clinical perspectives on thyroid cancer. N Engl J Med. 2016 Sep 15; 375(11): 1054-67. doi: 10.1056/NEJMra1501993
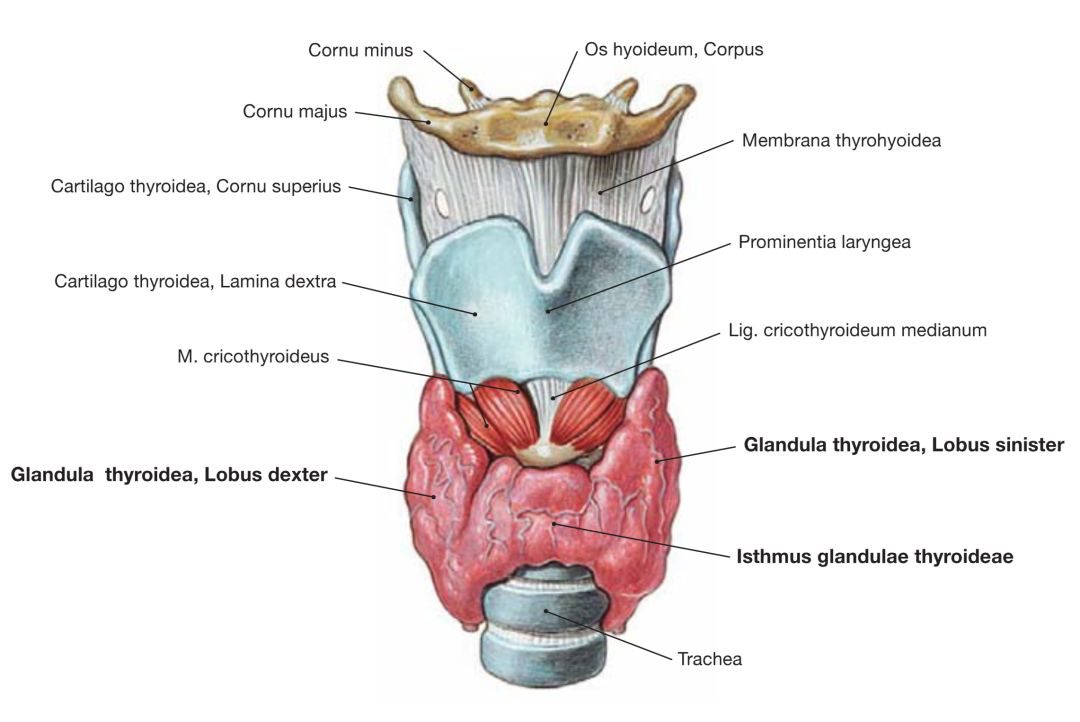
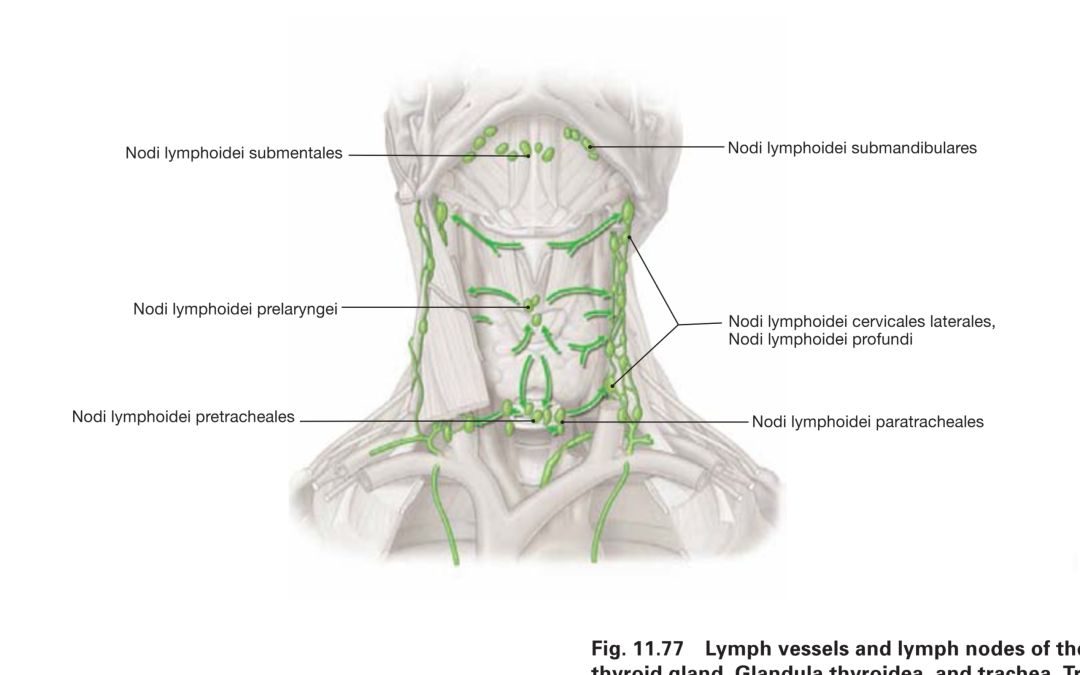
[2] F. Paulson & J. Waschke. (2011). Sobotta Atlas of Anatomy Latin Nomenclature, General Anatomy and Musculoskeletal System, 15th Edition. URBAN & FISCHER, Miinchen. pp.192, Fig 11.51; pp.207, Fig 11.77.
[3] Vaccarella S, Dal MasoL, Laversanne M, et al. (2015). The impact of diagnostic changes onthe rise in thyroid cancer incidence: a population-based study in selectedhigh-resource countries. Thyroid. 2015 Oct;25(10):1127-36. doi:10.1089/thy.2015.0116.
[4] Grani G, Lamartina L, Montesano T, et al. (2018). Lack of association between obesity and aggressiveness of differentiated thyroid cancer. J Endocrinol Invest. 2018 Apr 17. doi: 10.1007/s40618-018-0889-x.
[5] Cabanillas ME, McFadden DG, Durante C. (2016). Thyroid cancer. Lancet. 2016 Dec 3; 388(10061): 2783-2795. doi: 10.1016/S0140-6736(16)30172-6.
[6] Lamartina L, Grani G, Durante C, et al. (2018). Follow-up of differentiated thyroidcancer –what should (and what should not) be done. Nature Reviews Endocrinology, publishedonline 01 Aug 2018. doi: 10.1038/s41574-018-0068-3.
[7] Tuttle RM, Haugen B, Perrier ND. (2017). Updated American Joint Committee oncancer/tumor-node- metastasis staging system for differentiated and anaplastic thyroid cancer (Eighth edition): what changed and why? Thyroid. 2017Jun; 27(6):751-756. doi: 10.1089/thy.2017.0102.
[8] Kim TH, Kim YN, Kim HI, et al. (2017). Prognostic value of the eighth edition AJCCTNM classification for differentiated thyroid carcinoma. Oral Oncol. 2017Aug; 71:81-86. doi: 10.1016/j.oraloncology.2017.06.004.
[9] Pontius LN, Oyekunle TO, Thomas SM, etal. (2017). Projecting survival in papillary thyroid cancer: a comparison of the seventh and eighth editions of the American Joint Commission on cancer/union for international cancer control staging systems intwo contemporary national patient cohorts. Thyroid. 2017 Nov; 27(11): 1408-1416. doi:10.1089/thy.2017.0306.
[10] Links TP, vanTol KM, Jager PL, et al. (2005). Life expectancy in differentiated thyroid cancer: a novel approach to survival analysis. Endocr Relat Cancer. 2005 Jun; 12(2):273-80. doi:10.1677/erc.1.00892.
[11] Durante C, MontesanoT, Torlontano M,et al. (2013). Papillary thyroid cancer: time course of recurrences during postsurgery surveillance. J Clin Endocrinol Metab. 2013Feb;98(2):636-42. doi: 10.1210/jc.2012-3401.
[12] Haugen BR, Alexander EK, Bible KC, et al. (2016). 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on thyroidnodules and differentiated thyroid cancer. Thyroid. 2016 Jan; 26(1):1-133. doi:10.1089/thy.2015.0020.
[13] Verburg FA, M?der U, Reiners C, et al. (2014). Long-term survival in differentiated thyroid cancer is worse after low-activity initial post-surgical 131I therapy in bothhigh- and low-risk patients. J Clin Endocrinol Metab. 2014 Dec;99(12): 4487-96.doi: 10.1210/jc.2014-1631.
[14] Ho AL, Grewal RK, Leboeuf R,et al. (2013). Selumetinib-enhanced radioiodine uptake inadvanced thyroid cancer. N Engl J Med. 2013 Feb 14;368(7):623-32. doi:10.1056/NEJMoa1209288.
[15] Leboulleux S, Girard E, Rose M, et al. (2007). Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J Clin Endocrinol Metab. 2007 Sep;92(9): 3590-4.doi: 10.1210/jc.2007-0444.
[16] Shin JH, Han BK, Ko EY. (2007). Sonographic findings in the surgical bed after thyroidectomy: comparison of recurrent tumors and nonrecurrent lesions. JUltrasound Med. 2007 Oct; 26(10):1359-66.
[17] Lamartina L, Deandreis D, Durante C, et al. (2016). Endocrine tumours: imaging in the follow-up of differentiated thyroid cancer: current evidence and future perspectives for arisk-adapted approach. Eur J Endocrinol. 2016 Nov;175(5): R185-202. doi:10.1530/EJE-16-0088.
[18] Tuttle RM, Tala H, Shah J, et al. (2010). Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnantablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010Dec; 20(12):1341-9. doi: 10.1089/thy.2010.0178.
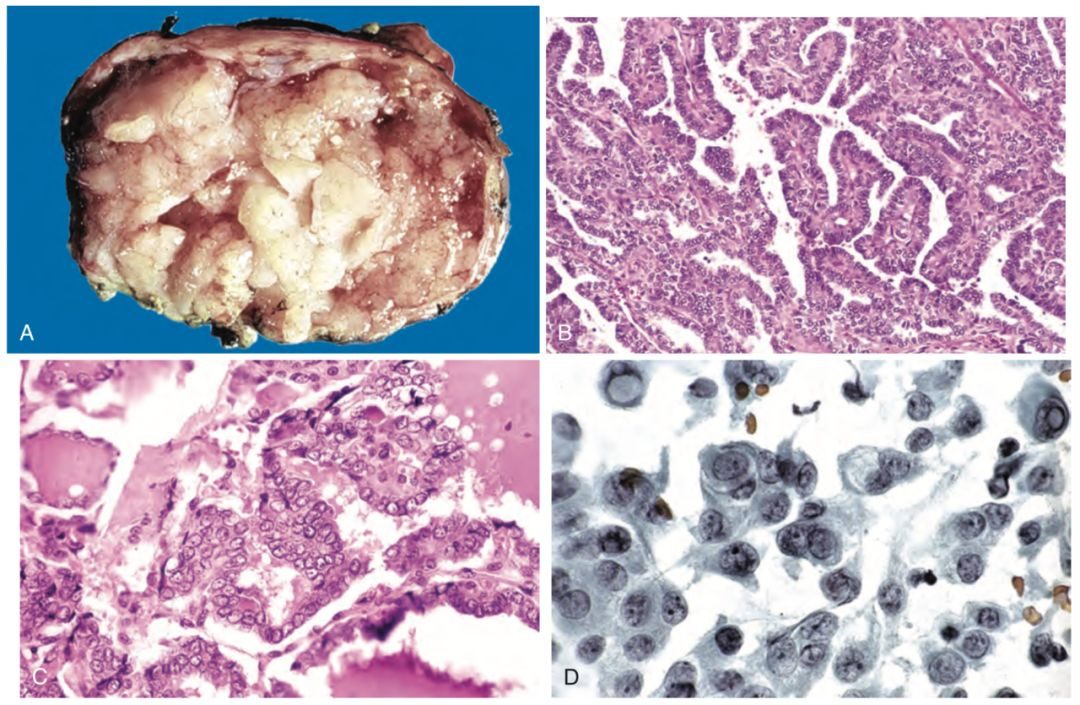
[19] Vinay Kumar, Abul K. Abbas, Jon C. Aster. (2015). Robbins and Cotran Pathologic Basis of Disease, 9th Edition. ELSEVIER SAUNDERS, Philadelphia, PA. pp. 1096, Fig 24-19; pp.1097, Fig 24-20.
[20] Ye L, Zhou XY, Huang FJ, et al. (2017). Corrigendum: the genetic landscape of benign thyroid nodules revealed by whole exome and transcriptome sequencing. Nat Commun. 2017 Jun 5;8:15533. doi: 10.1038/ncomms15533.
原文鏈接:
@all 上周的「內分泌醫生生存現狀調研」已經結束,小編隨機抽取了3名參與調研的用戶,每人贈送《約翰·霍普金斯糖尿病指南:糖尿病的治療與管理》一本。這3名獲獎者的手機號是:189XXXX1965、137XXXX0006、180XXXX9680,恭喜!








漲姿勢了請點贊▼